Does DIEP flap breast reconstruction increase the risk of breast cancer recurrence?
Patients choosing to undergo breast reconstruction are often concerned that their decision may increase their risk of breast cancer recurrence. A recent study published in the British Journal of Surgery looked at the risk of recurrence specifically after DIEP flap reconstruction.
The study compared 250 patients who had DIEP flap reconstruction between 1999 and 2013 with more than 700 control patients. Breast cancer recurrence was seen in over 19 percent of patients who had DIEP flap surgery and over 23 percent of patients in the control group. Interestingly, the 5-year breast cancer-specific survival rate was highest in patients having DIEP flap surgery after 2008 – 92.4 percent in the DIEP flap group versus 87.4 percent in the control group.
The study design does raise some questions about selection bias. For example, all DIEP flap procedures in this study were performed at least 24 months after mastectomy. No DIEP flaps were performed at the same time as the mastectomy (‘immediate’ reconstruction). In addition, a larger number of patients in the DIEP flap group than the control group received adjuvant therapy.
While the survival rates between groups may have been influenced by patient selection, this study shows that patients with breast cancer undergoing DIEP flap breast reconstruction do NOT have a higher rate of breast cancer recurrence than patients undergoing mastectomy alone.
Breast Advocate Founder Presents at Male Breast Cancer Coalition’s Annual Conference
According to the American Cancer Society, about 2,670 new cases of invasive male breast cancer will be diagnosed in 2019 and about 500 men will die because of this diagnosis.
Male breast cancer is rarely discussed in breast cancer awareness campaigns. The Male Breast Cancer Coalition (MBCC) aims to change this. Their mission is to build awareness of male breast cancer through the wisdom and experiences of survivors through speaking arrangements, social media and their annual conference.
This year, Breast Advocate founder, Dr. Minas Chrysopoulo, was honored to join the MBCC at their annual conference last weekend to discuss male breast reconstruction options. “Like women, men can experience the same concerns about their appearance following breast cancer surgery, most commonly a mastectomy,” shares Dr. Chrysopoulo. “Knowing there are reconstructive options is a great relief to some male breast cancer patients.”
Male breast reconstruction can include several different procedures…
Fat grafting is the most commonly performed method of reconstruction in male breast cancer patients. The procedure is performed by removing fat (using liposuction) from one area of the body, purifying it, and re-injecting it into the chest to fill in chest contour deformities.
A small breast implant can be used to reconstruct a male breast after a mastectomy. Since the aesthetics of the male breast are usually much different to that of woman, a custom implant is often the best choice for the best symmetry.
Some patients can have extensive chest wall deformity following breast cancer treatment, especially if part of the pectoral muscle is removed because of tumor involvement. In these situations, an autologous flap (reconstruction using the patient’s own tissue) may be a good option. Flap options include a Latissimus Dorsi (or “lat”) flap which uses (part or all) of the back muscle below the shoulder blade along with a segment of overlying fat and skin, or the DIEP flap which uses skin and fat from the lower abdomen.
Nipple reconstruction can be performed on its own or in conjunction with any other reconstructive procedure. If desired, the reconstructed nipple and areola can later be tattooed for a more natural appearance.
- Scar Revision Surgery
Scar revision can improve the appearance of breast surgery scars after mastectomy or lumpectomy and can be used in conjunction with fat grafting to improve chest contour defects. Releasing tethered scars can also help reduce discomfort.
- Tattooing
Various forms of tattooing can be performed along with other reconstructive procedures. These include:
- A nipple-areola tattoo (2D or 3D), either alone or in conjunction with nipple reconstruction
- An ornamental tattoo covering the surgical site
Male breast reconstruction (regardless of the procedure) is usually performed after completion of all breast cancer treatment. In select cases, it can be performed at the same time as the mastectomy.
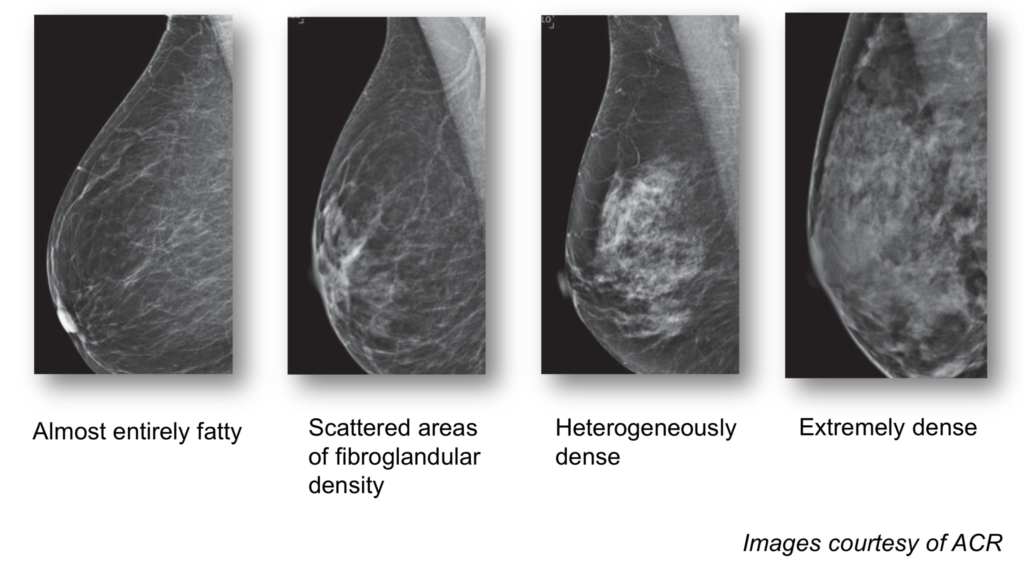
Why you Need to Know Your Breast Density
A recently passed law means that for the first time in over 20 years, the FDA is updating regulations for mammography screening to give patients more information about their breasts. The amendments will specifically require that patients be informed of their breast density in all U.S. states.
Breast tissue that is more fatty in consistency appears dark gray or even black on a mammogram, which makes it fairly easy to identify a breast cancer since that appears as a white lesion on mammograms. Dense breast tissue consists mostly of glandular tissue and is not fatty at all. Glandular tissue also appears white on a mammogram making it harder to detect a cancer. Dense breasts can therefore mask a breast cancer.
Younger women are much more likely to have dense breasts than older women. As women approach menopause, the glandular tissue is gradually replaced by more fatty tissue.
About 50% of women in the U.S. have dense breasts. Women with the densest breasts are up to six times more likely to develop breast cancer than women with fatty breasts. Once diagnosed, a woman with dense breasts may have an increased chance of developing aggressive or metastatic breast cancer, which decreases her overall chance of survival.
The FDA will now require mammography centers and radiologists to share the patient’s breast density information on the mammogram report, in easy understandable language, along with how it might influence the accuracy of the mammogram. Women with dense breasts have additional screening options including 3D mammography, breast ultrasound, and MRI.
The new law is a major victory for the patient advocacy movement, in particular AreYouDense.org, founded by the late Nancy Capello, PhD. Dr Capello was responsible for the first state-based density reporting law passed in Connecticut in 2009 and spearheaded efforts to standardize the communication of dense breast tissue nationally through changes in the Mammography Quality Standards Act.
Reports of Breast Implant-Related Illnesses Prompt FDA Review
New safety concerns over breast implants has prompted the FDA to hold a two-day meeting to hear from researchers, patients, plastic surgeons, and implant manufacturers. The hearing was scheduled for March 25th and 26th, 2019.
Concerns surfaced recently following the publication of the first study to review breast implant safety data following the FDA’s approval of silicone implants. The study, published in Annals of Surgery, is the largest ever study of silicone breast implants.
The researchers analyzed data on nearly 100,000 patients enrolled in the study between 2007 and 2010. More than 80,000 patients received silicone implants (Allergan or Mentor); the rest received saline implants. Seventy-two percent of the patients underwent primary breast augmentation, 15 percent had revision augmentation, 10 percent had primary breast reconstruction, and three percent had revision reconstruction procedures.
The authors found silicone implants are generally safe but are also associated with a slightly higher risk of a few rare diseases including Sjogren’s syndrome (8-fold increase), scleroderma (7-fold increase), rheumatoid arthritis (6-fold increase), stillbirth (4.5-fold increase), and melanoma (4-fold increase). One case of BI-ALCL (rare lymphoma associated with textured implants) was reported.
The findings have been disputed by many experts, including federal health regulators, who nevertheless scheduled the public meeting to consider implant safety.
“These findings aren’t meant to suggest implants caused these problems,” said Dr. Mark Clemens, an MD Anderson professor of plastic surgery, Breast Advocate App contributor, and the senior investigator of the study. “They’re associations, which underscore the need for more research in this area, but do provide key safety information for women and their providers to consider when thinking about cosmetic or reconstructive surgery with breast implants.”
Since the publication, the FDA has also issued a statement acknowledging that implantable devices, including breast implants, may make some people sick. “A growing body of evidence suggests that a small number of patients may have biological responses to certain types of materials in implantable or insertable devices… [which can include] inflammatory reactions and tissue changes causing pain and other symptoms that may interfere with their quality of life.”
Following the hearing and consideration of all the information presented, the FDA released this statement.
Robotic Mastectomy – a natural evolution or a huge safety concern?
Robotic nipple-sparing mastectomy was first described in 2015 and appears to be gaining traction in Europe. Slower to catch on in the US, the procedure is now also starting to raise safety concerns for some surgeons.
The da Vinci robot is not yet FDA-approved for mastectomy. There is concern amongst some medical professionals that robotic tumor removal could inadvertently cause breast cancer cells to spread by fragmenting the cancerous tissue as it is being pulled out of the small incision.

Dr Hooman Noorchashm, a Philadelphia-based surgeon turned patient advocate, has raised questions about the safety and appropriateness of using the da Vinci robot for mastectomies… “The reason why I am focused on robotic mastectomy is because I think there is a parallel [with hysterectomy via power morcellator] of selling cosmesis and convenience to women for a surgical operation. The US Food and Drug Administration (FDA) has a history of being lax in its oversight of 510K devices, which include the power morcellator and the da Vinci robot, he said. These devices can replace established standards of care without proper evidence.”
To date there have been no clinical trials to compare the safety of robotic surgery with the traditional techniques used for breast cancer surgery.
Dr Noorchashm has also referred to a recent study from MD Anderson that compared survival rates of laparoscopic hysterectomies for cervical cancer to traditional “open” surgical methods that use larger incisions. The research found that patients who underwent the minimally invasive laparoscopic surgery were four times more likely to experience recurrence than those who had the open surgery. These finding came over 10 years after laparoscopic surgery was recommended as the standard for care.
This is not to say that robotic surgery isn’t an option for some patients. Recent headlines have praised surgeons for performing robot-assisted prophylactic breast surgery and immediate implant-based breast reconstruction. Although controversial, there is no evidence to suggest robotic surgery could increase the risk of developing breast cancer in preventative mastectomy cases.
Long-term, high quality research is underway, but it could be years before there is a better understanding of the full impact and risk of robotic surgery for breast cancer patients.
Looking for more information to help you weigh your surgical options? Download the Breast Advocate app now.
Addendum 2/28/19:
FDA issues safety communication about robotic mastectomies – Caution When Using Robotically-Assisted Surgical Devices in Women’s Health including Mastectomy and Other Cancer-Related Surgeries.
How Patient Advocacy and Shared Decision-Making are Changing Breast Cancer Care
The rise of patient advocacy and shared decision-making are transforming breast cancer care.
Shared decision-making is a process whereby the patient and physician participate in the medical decision-making process together. The approach considers all evidence-based treatment options and associated risks, the physician’s expertise, together with the patient’s preferences, values and expectations to arrive at the best treatment plan for the patient. Multiple studies show this collaborative approach improves patient outcomes and satisfaction.
Empowered, self-educated patients are increasingly advocating for themselves, seeking to have a greater voice in their treatment planning. As the only shared decision-making breast cancer app in the World, Breast Advocate® is very proud to be able to facilitate the patient advocacy movement.
Now, patient advocacy is also making positive strides in the research arena. Nowhere has this been more evident than at the 2018 San Antonio Breast Cancer Symposium last month, where patients have become an integral part of the meeting. By participating on panels, asking questions and weighing in on research, patients have “shifted the direction of breast cancer research,” says Dr. Elaine Schattner. “By speaking up, advocates at the meeting have shifted the direction of breast cancer research. Some are alive, improbably, as a consequence of new treatments enabled and promoted by their advocacy.”
Collaboration can only make things better. We look forward to patient advocates having a constant seat at the table at many more scientific meetings!
New Law in California Makes Finding a Plastic Surgeon Safer
Patients researching their healthcare options are often told to ensure their physician is “board certified”. This is particularly important in the case of surgery since there is actually no law that prevents a physician, regardless of training, from performing any procedure. This loophole is often exploited by “cosmetic surgeons” who have never received any formal plastic surgery training.
The Medical Board of California (MBC) today unanimously voted against allowing members of the American Board of Cosmetic Surgery (ABCS) to advertise as “board certified” cosmetic surgeons. This is because the ABCS is not a member of the American Board of Medical Specialties (ABMS).
This means that only plastic surgeons certified by the American Board of Plastic Surgery (ABPS) can claim to be board-certified plastic or cosmetic surgeons, as the ABPS is the only plastic surgery board acknowledged by the National Board of Medical Specialties.
While breast reconstruction is not a ‘cosmetic’ procedure, it is a type of plastic surgery. For patients seeking breast reconstruction, finding a plastic surgeon who is board-certified by the ABPS ensures they have the expert training and experience required to perform breast surgery safely.
“This is, frankly, a tremendous relief. California has a large number of cosmetic surgery patients and the most ABCS members of any state, which means it holds the greatest potential for those patients to be misled by advertisements that a doctor is a ‘board certified surgeon’,” says American Society of Plastic Surgeons President Alan Matarasso, MD, FACS in the latest news report coming from ASPS. “Today’s ruling means those patients are less likely to choose a particular provider because they were exposed to a confusing ad. That’s going to make patients safer. Our specialty owes a huge debt of gratitude to all the plastic surgeons who invested their time and talents to help protect our patients.”
Now if only other states would follow suit…
Immune System Cancer (BIA-ALCL) Linked to Some Types of Breast Implants
The FDA has announced that breast implants have been linked to a certain type of non-Hodgkin’s lymphoma (cancer of the immune system) known as Breast Implant-associated Anaplastic Large Cell Lymphoma (BIA-ALCL).
About 450,000 breast implant procedures (cosmetic and reconstructive) are performed yearly in the US alone. So far, 626 cases and 17 deaths have been reported globally. As of September 30, 2018, the FDA had received a total of 660 medical device reports (MDRs) of BIA-ALCL, including 9 patients who died in the US. These numbers are being updated frequently as more cases are diagnosed. Published data on lifetime risk of developing this lymphoma from a breast implant varies widely, between 1 in 1,000 and 1 in 30,000. This risk may vary among different implant manufacturers. The risk is higher when the implants have a rougher surface (have “aggressive texturing”) than when they have less rough surface.
Two types of breast implants are used for cosmetic augmentation and breast reconstruction: smooth surfaced and textured. Textured surfaces were introduced to encourage tissue adherence to prevent implants rotating. Currently, all anatomic-shaped implants on the market are textured. Round implants are available as both smooth and textured devices.
Most studies report BIA-ALCL is exclusively associated with textured implants. There have been no confirmed cases developing in patients who have only had smooth implants. However, the FDA has not excluded this possibility. There is no doubt the highest risk is associated with the more aggressively textured devices and polyurethane implants.
Symptoms include a large fluid collection developing more than one year after receiving an implant, breast swelling, a breast mass or new onset of breast asymmetry.
“Patients with BIA-ALCL most often develop the disease within eight to ten years of having a textured breast implant placed,” says Dr Mark Clemens, a leading global authority on BIA-ALCL and expert contributor to the Breast Advocate App. “Some patients may have a lump in the breast or armpit. Some patients developed an overlying skin rash or hardening of the breast. Women who develop these symptoms should see their physician to be evaluated with a physical exam and may require further testing… Patients without symptoms do not need to be tested for BIA-ALCL.”
In terms of testing, Dr Clemens explains “patients may receive an ultrasound or a magnetic resonance imaging (MRI) of an enlarged breast to evaluate for fluid or lumps around the implant. If fluid or a mass is found, patients will require a needle biopsy to test for disease. A fine needle biopsy is performed in a clinic by their physician or by an interventional radiologist using ultrasound guidance. Needle biopsies do not require surgery. The biopsy draws fluid from around the implant. This fluid is then tested for CD30 immunohistochemistry (CD30 IHC) by a pathologist. This is the screening test for BIA-ALCL and may take a week for evaluation. CD30 IHC is a common test, can be performed in any hospital and pathology lab, and does not require a specialized center. Some community hospitals may send specimens to a larger academic hospital if the lab results are confusing, suspicious, or indeterminate. Testing for CD30 IHC is required to make a diagnosis or rule out BIA-ALCL and is covered by all health insurance programs because the test is an investigation of a possible cancer.” Fluid collections around a breast may happen without BIA-ALCL and are called seromas. Once BIA-ALCL has been ruled out, a physician can treat a seroma as they normally would.
Early diagnosis and appropriate, prompt treatment including excision of the implant capsule are associated with very high cure rates. Disease re-occurrence is rare after surgical removal for early disease. Some patients can develop metastatic disease, in which case chemotherapy either alone or in combination with immunotherapy, is recommended.
According to the FDA and American Society of Plastic Surgeons, in the absence of any symptoms, there is no need to remove textured implants due to the risk of developing BIA-ALCL at this time. However, patients who are unhappy with their implants do have other options. These include implant revision surgery, or replacement of the implant with the patient’s own tissue (fat grafting or flap surgery).
Immunotherapy Improving Treatment of Triple Negative Breast Cancer
Triple-negative breast cancer is so called because, unlike more common forms of breast cancer, its cells do not have receptors for estrogen, progesterone, or the HER2 protein.
Triple-negative cancer makes up only about 10-15% of diagnosed breast cancers, but is one of the most aggressive and deadly forms of the disease. It is also more likely to affect younger women under 50. In most cases, triple-negative tumors quickly become resistant to chemotherapy and spread to other parts of the body.
Over the last few years, immunotherapy — a treatment that boosts’ the body’s defenses against infection and diseases — has been gaining ground as a potential therapy for several different types of cancer, including breast cancer.
A recent phase 3 study, published in the New England Journal of Medicine, included over 900 women in 41 countries randomly assigned to one of two treatment groups: one group received the immunotherapy drug atezolizumab (a monoclonal antibody drug) together with chemotherapy, the other group was given a placebo with chemotherapy.
“In a combined treatment approach, we are using chemotherapy to tear away the tumour’s ‘immune-protective cloak’ to expose it as well as enabling people’s own immune system to get at it” said lead author of the study, Professor Peter Schmid.
Patients who received the immunotherapy drug along with chemotherapy extended overall survival by 10 months, reducing the risk of death or disease progression by up to 40%.
Breast Advocate Founder Moderates Shared Decision-Making Panel At ASPS ‘The Meeting’
Breast Advocate’s Founder Dr. Minas Chrysopoulo this month had the honor of moderating a panel on the importance of shared decision-making in breast reconstruction at this year’s American Society of Plastic Surgeons (ASPS) annual meeting in Chicago. ‘The Meeting’ is the largest plastic surgery meeting in the World and welcomes surgeons from all over the globe. Dr Chrysopoulo had the privilege of being joined on the panel by Breast Advocate co-contributor Dr Hani Sbitany, and patient advocates Terri Coutee and Kirstin Litz.
“Once upon a time, I’d tell a patient their breast reconstruction options and the associated risks and recommend what I thought was best. Then I discovered shared decision-making and it changed my practice forever,” shared Dr. Minas Chrysopoulo.
What exactly is “shared decision-making”?
Shared decision-making is the conversation and information exchange that happens between a patient and their healthcare professional to reach a treatment plan together. The doctor ensures the patient is fully educated about all their treatment options and the associated risks, while the patient shares their preferences, values and any other personal factors that are important in reaching the best plan for the patient.
Shared decision-making flies in the face of the paternalistic approach to healthcare delivery and instead empowers patients to have an equal voice in their treatment planning – It was the driving philosophy behind the creation of the Breast Advocate App.
Listen to the entire shared decision-making presentation here.


